

Sacramento Care Model Improves Multiple ED Operations Metrics in a High-Volume ED
William D. Browder, MD, FACEP | Ralph Rosignolo, RN, BSN | Jason Morgan, RN,BSN | Melissa Escano, BS | MIke Marra, BS
Sentara Healthcare, Norfolk, VA
Jamil Bitar, MD, FACEP | Maurice Makram, MD, FACEP
UBQ Corporation, Sacramento, CA

Description: Sentara Leigh Hospital a 70,000 Plus visit ED in Norfolk Virginia, developed and implemented a care delivery model based on lesson learned from a Kaiser South Sacramento based Emergency Department. After introduction through an IHI Patient Flow conference. Sentara Healthcare began collaboration with the Kaiser ED Leadership team from the Sacramento area to learn from their recognized best practice model for high volume emergency department patient flow based on LEAN concepts. Sentara Leigh took key concepts from the Sacramento care model to develop a six-phase implementation plan. This plan includes Team and acuity based zone care, rotational assigned patient flow utilizing a cloud based software system or PASS, Demand capacity matching nursing and provider resources into convert ED operations to this new model over a four month period.
Results: During 2016, Sentara Leigh Hospital treated 70,497 patients versus 67,890 in 2015.
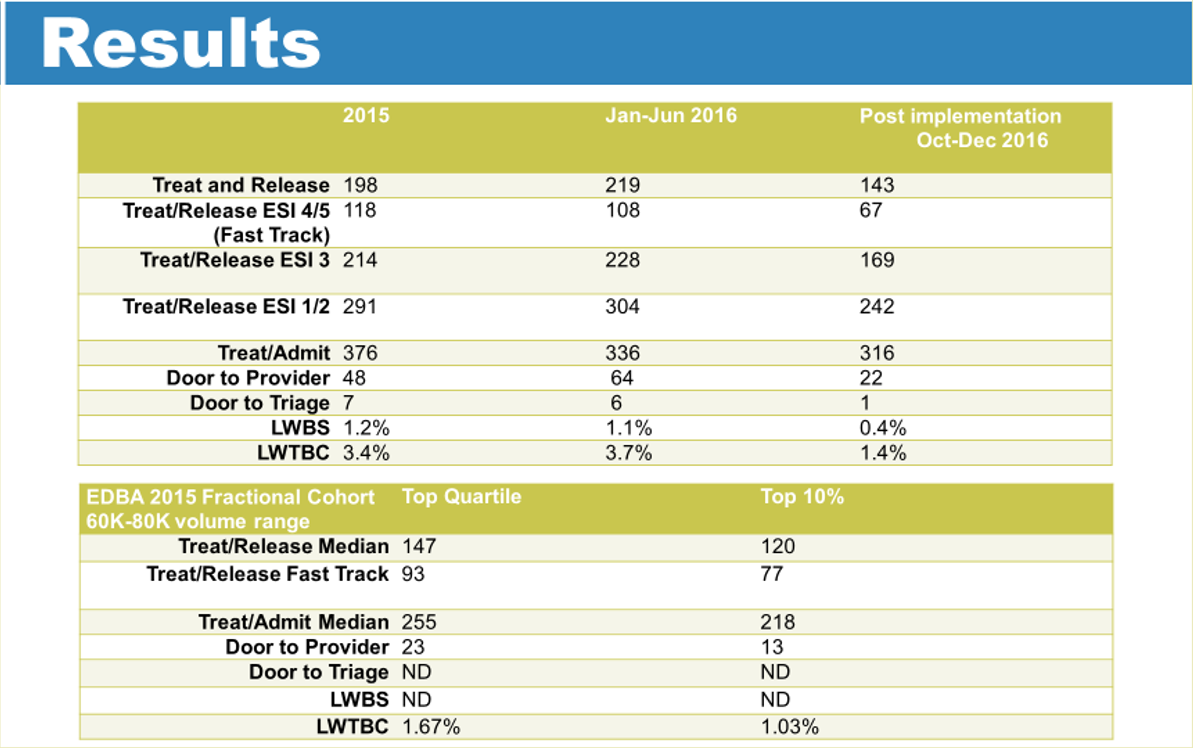
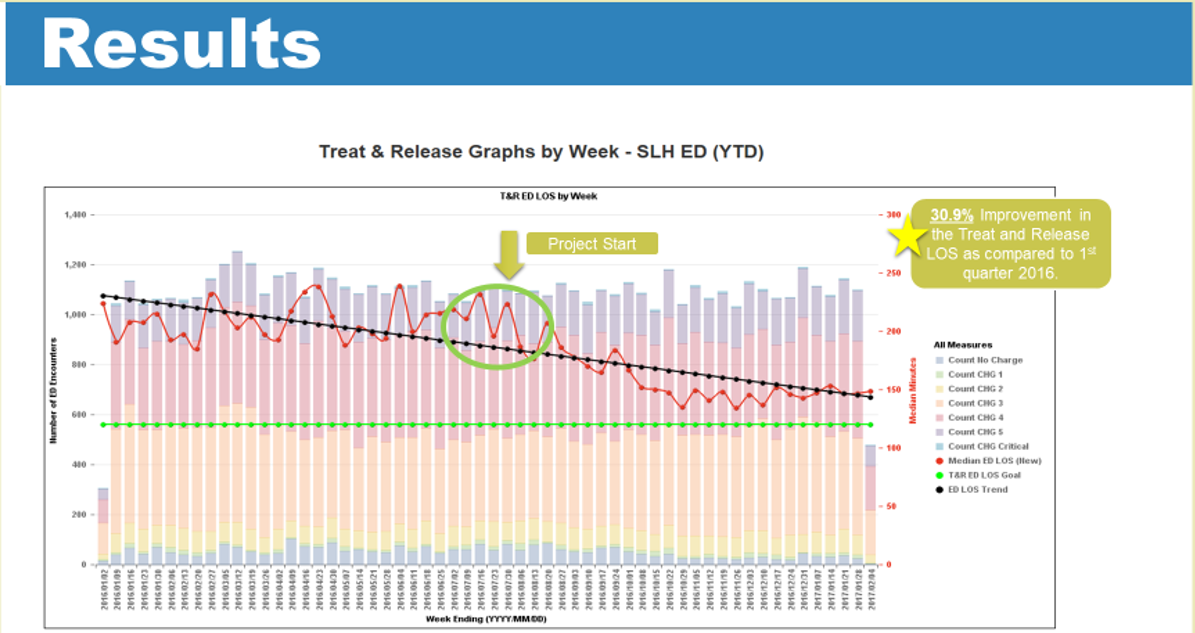
The Median Treat and release time in 2015 was 198 median minutes, in the first 6 months of 2016 it was 219 median minutes, and in the last 3 months of 2016 after full implementation it was 143 median minutes.
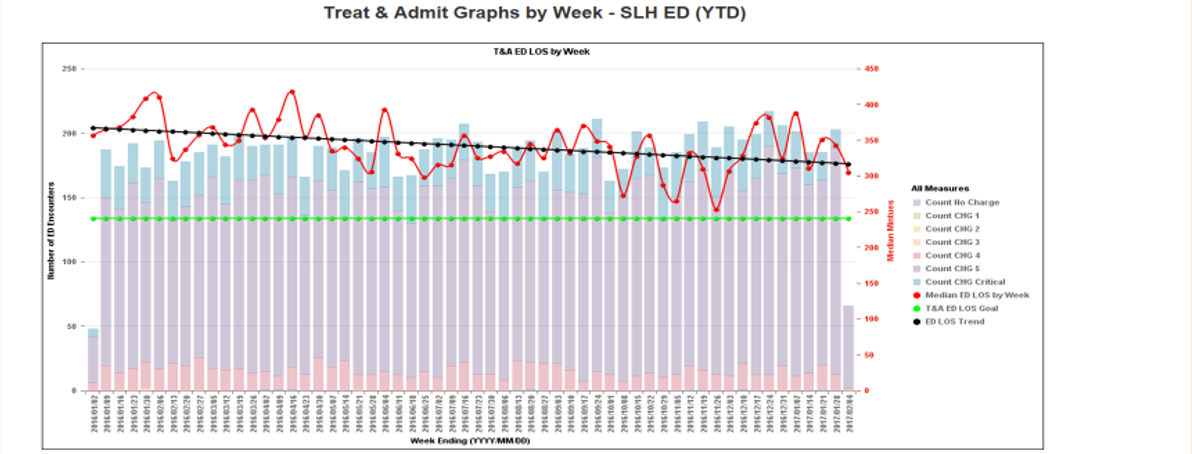
Treat and Admit times in 2015 were 376 median minutes. first half of 2016 were 336 median minutes, and after full implementation were 316 minutes.
LWBS was 1.2% in 2015, in the first 6 months of 2016 was 1.1 %, and in the last 3 months of 2016 after full implementation was 0.4%.
LBTC was 3.4% in 2015, 3.7% in first 6 months of 2016, and 1.4% after full implementation. Treat and release times for ESI 4/5 patients improved from 118 median minutes to 67 median minutes after implementation of the Fast track synchronized work process.
Treat and release times for ESI 3 patients improved from 214 median minutes to 169 median minutes after implementation of focused care teams. Treat and release times for ESI 1/2 patients improved from 291 minutes lo 242 median minutes after implementation of acute care teams.
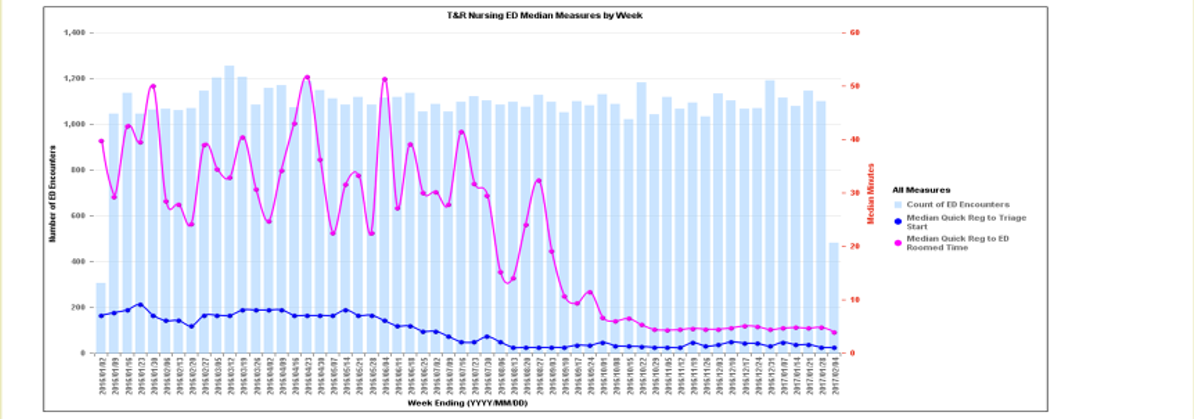
Door to provider improved from 48 minutes to 22.9 minutes after initiation of team assignment system software, PASSsm. Door to triage improved from 2016 baseline of 7 median minutes to 1 median minute after PIVOT.
Volume increased after full implementation from 193 patients per day to 200 patients per day despite volume losses at similar Sentara ED’s in the region.
Early Trends show reduction in lab and radiology testing per patient compared to baseline which we feel is due to elimination of pre-emptive testing. Sentara Leigh is a space constrained Facility that saw 5.14 visits per square foot and 2400 visits per bed in 2016.
Lessons Learned: The Sacramento patient flow model is a novel approach to emergency medicine operations based on LEAN concepts. Core Components include a no-wait culture, ownership of patient flow through team assignments and load balancing using the Patient Assignment and Sorting System (PASSsm), a three acuity zoned and modular team care approach, eliminating wasfe and unneeded front end care, and the concept of synchronized work. Several aspects of the model such as eliminating all pre-emptive testing, nurses and providers assessing patients simultaneously, and using cloud bases rotational assignment software through PASSsm, to route and assign patients are not commonly used in ED operations. Placing providers and nurses in small teams and using acuity bases care zones increases efficiency and ownership of patients. The successes at several Kaiser Sacramento EDs were reproducible at Sentara Leigh. Sentara Healthcare believes this care model can succeed at all high volume ED’s and produce similar gains. Furthermore, it can be installed in a modular fashion. Sentara will begin a 12-month period to transition all Eds in our system with volume greater than 40K to this care model using the template developed at Sentara Leigh. Sentara will further refine operations utilizing ongoing LEAN concepts.

Sentara Leigh Hospital, a 35 bed Emergency department in Norfolk, VA, faces many flow struggles commonly found in busy emergency departments around the country. Sentara Leigh treated 67,890 patients in 2015 and had a visit/space ratio of 1939, which would rank 82 out of 102 ED’s reporting this metric in the 60,000 – 80,000 EDBA Cohort. During the 2015 year Sentara Leigh was below EDBA Cohort average in LWBS, LBTC, Door to Provider, and Treat and Release times. A system commitment to improve operations led us to seek out collaboration with another health system that was using novel approaches to improve ED care. The goal was to improve ED operations at Sentara Leigh to top quartile in the EDBA cohort database and use lessons learned from performance improvement at Sentara Leigh to improve ED operations at all Sentara emergency departments.
After introduction through an IHI Patient Flow conference, Sentara Healthcare began collaboration with the Kaiser ED Leadership teams from the Sacramento area to learn from their novel best practice model for high volume ED patient flow. Kaiser Sacramento based Emergency Departments in particular have utilized LEAN Strategies, zoned team based care, and rotational, acuity based, assigned patient flow to create a Novel care model.
This model focuses on vertical care, appropriate use of limited bed space, ownership of patients by providers and teams upon entry, and simultaneous nursing and provider work to improve operational efficiency. This model also is driven by a cloud based Rotational Team assignment protocol utilizing the Patient Assignment and Sorting System (PASS) to Load balance and manage flow. Kaiser Sacramento Emergency Departments have been able to achieve near national best practice results on numerous operational metrics using this model.
Over a four-month period, Sentara Leigh Hospital Developed and Implemented a multi phased, modular, process improvement approach utilizing core concepts based on the Sacramento model and lessons learned. A well-defined process improvement plan and a dedicated process improvement support team assisted in each implementation phase of the model. Prior to implementation, nursing and provider staffing underwent a detailed demand capacity Analysis. Combined nursing and provider zoned care teams models where established. Core members were taught key principles of team approach care. Each Care team works utilizing SWARM (Synchronized Work And Rooming Method) that was developed at Kaiser during which nursing and provider work is done simultaneously. With this process all pre-Emptive testing was eliminated. All staff is encouraged to have the patient only tell the story once and perform most needed tasks simultaneously. The focus was shifted on getting patients in front of provider nurse teams to perform all needed work and assessments.
The Sacramento model modular implementation is composed of six phases
- PIVOT Triage
- Demand Capacity Analysis/Matching nursing and provider resources
- Fast Track (ESI 4/5 now) low acuity team
- Patient Assignment and Sorting System (PASS) driven flow using cloud base software provider UBQ
- Focused care middle acuity Teams (ESI 3 flow)
- Acute Care Teams (ESI 1/ 2 flow and complex ESI 3 flow)

- Identify a novel ED operations model with proven success to use as a framework to drive performance improvement
- Implement a team based care concept to improve core operational metrics at Sentara Leigh with goal of top quartile performance in EDBA volume cohort
- LWBS and LWTBC
- Door to Triage
- Door to Provider
- Treat and Release median time
- Treat and Admit Median time
- Develop a Reproducible model to implement process improvement in similar volume ED’s

Fast Track ESI 4/5 Care Team
Manages all ESI 4/5 Flow. Nurse, Provider, ED tech assess and treat assigned patients as a team utilizing one room placed a point of entry and 1 procedure room and results waiting area. Approximately 50% of patients are dispositioned by the team as a one step process from the assessment room. Common procedures are performed in a procedure room that has pre-packed kits to expedite care of common complaints. Strong LEAN concepts are utilized to reduce non-value added work. Flow is managed utilizing the PASS system with a rolling hourly cap of 5 patients per hour to promote efficiency and manage bonuses. Team are expected to see up to 26 patients in an eight-hour shift.
Focused Care ESI 3 Teams
Manages majority of ESI 3 flow. Nurse, provider, Tech teams assess ESI 3 patients as a team at point of entry utilizing 2 intake rooms adjacent to waiting room. Patients are assigned via PASS on a rotational basis and flow is controlled utilizing a rolling cap. After initial assessment and initiating treatment and obtaining labs, needed further ancillary testing or procedures are performed. A vertical care area supports the teams along with a 7-bed treatment area. Each area is supported by nursing resources. Any patient deemed to be too complex is escalated to the acute Care teams. Each Team is expected to see up to 20 patients in an eight-hour shift.
Acute Care High Acuity teams
Each team is made up of 2-3 nurses, one ED tech, and one provider supported by 8 beds with on critical care bed and 2 hall spaces. ESI 1,2, and complex or non-ambulatory ESI 3 Patients are assigned via PASS on a rotational basis. Teams sit in common work area and constantly communicated about needed care, bed utilization, and future care plan. Each shift starts with a “Fast Start” protocol where they will get three patients in a row. Patients are seen in SWARM on intake where nurse and provider and tech perform simultaneous provider intake, nursing assessment and intake, completion vital signs, and obtain needed diagnostics and treatment. Teams own that patient and pull to available treatment space to see next patient with goal to room and see all patients in 20 minutes or less. Bed management becomes core concept of teams. Planning ahead to find space to see next patient and ownership of flow in team are primary objectives. Because team shifts are aligned, all team members are strongly motivated to progress care as fast and efficiently as possible. Long Length of stay patients and psychiatric cases can be moved to a 5-bed observation area to maintain flow.
ESI based Demand Capacity/Team Staffing
With support of Pl team, we reviewed demand capacity curves for our ED based on total volume and ESI score. Appropriate team staffing was determined for each day of the week. We also took a “one hour ahead” approach with the idea of being ready to accept the bolus. Further, models projected volumes for “Busy” days which we defined as 70th and 90th percentile for day. We projected needed capacity to address these peak demands. Nursing and provider shifts were matched so that all staff are working towards a common goal of seeing all assigned patients.
PASSsm / Team Assignment System
Team Assignment system is a Rotational Assignment software platform developed by UBQ ED to assign patients to provider lead teams at the point of entry. UBQ has partnered with Kaiser and now Sentara to provide this service to multiple ED’s. This system uses the PASS sm (Patient Assignment and Sorting System) to assign and load patients to teams based on ESI Acuity, workload balancing rules, and shift protocols. While Queuing theory suggests that assigning patients may lead to longer waits, we found PASSsm to be a powerful tool to promote ownership and a culture of accountability and drive reduction in door to provider times and ED Length of Stay. It prevents provider “cherry picking” and allows providers to focus on managing flow assigned to their team. A text push notification system was also deployed via PASSsm to facilitate proactive planning by team members to start care as soon as the patients arrive. PASS uses a frontloading protocol and taper down approach to team workloads. Further, it sets both total shift caps and hourly bumpers for teams and providers that promotes flow and operations. PASS allows data driven protocols to be put into place to activate call teams.

- The Sacramento Care model is a novel ED operations system based on LEAN concepts that Utilizes three Acuity care zones that focus on nurse-provider teams driven by an assigned rotational patient software system or PASS.
- The Sacramento care model can be successfully deployed in a phased approach. This process was successfully performed in four months at Sentara Leigh
- By Deploying PIVOT and removing all pre-provider testing, front end/entry operations focused on effective sorting and routing to provider nurse teams and reduced door to provider.
- The Sacramento Care model promotes a culture of no wait emergency department care, having patients only tell the clinical story once on entry, and synchronized nursing and provider work or SWARM.
- Patient Assignment and Sorting System (PASS) software is an extremely effective tool to manage ED flow into care teams. Furthermore, it allows team ownership at point of entry allowing ownership of the waiting room. It also effectively load balances teams leading to improved operational efficiency.